Decentralization was a necessity for the conduct of the clinical trials during the Coronavirus Disease 2019 (COVID-19) pandemic. This new way of managing clinical trials became a more recognized concept during the past few years that needs further development and a regulatory framework.
The decentralized clinical trial (DCT) is defined by the Food and Drug Administration (FDA) as "a clinical investigation where some or all of the trial-related activities occur at a location separate from the investigator’s location." DCTs are divided into two categories based on the degree of decentralization, which can range from fully decentralized to partially decentralize. In the case of a fully DCT approach, all trial procedures are conducted remotely through digital means and supply delivery with no in-person visits required to the trial site, whereas a hybrid approach may include some decentralized trial activities combined with traditional trial procedures such as in-person visits via mobile clinicians or alternative sites.
Clinical trials are essential for drug development and improving the health of patients. The remote DCT approach was recommended for adoption during the pandemic, with the scope to facilitate participation in trials by offering maximum flexibility and convenience. Nevertheless, the DCT approach has been recognised to bring benefits, and there is an increased demand for conducting clinical trials remotely. Some of the benefits DCTs provide are presented in Image 1.

Image 1. Benefits of clinical trial decentralization
Hereinafter, the background of clinical trial decentralization, the current knowledge, and the future of DCTs will be described.
The desire to conduct fully or partially remote clinical trials has been supported by continuous technological advances despite the lack of a regulatory framework on this topic. The industry’s limited experience and the absence of corresponding infrastructure and regulatory guidelines slowed down DCT adoption.
Industry recommendations and best practices
The benefits of conducting remote clinical trials have been recognized over the last few years, especially during the COVID-19 pandemic. However, the challenges of implementing this approach compelled pharmaceutical companies, clinical research organizations, investigators, and technology companies to collaborate in order to accelerate the development of tools and methods for working with DCTs.
The first to issue relevant recommendations on DCTs is an organization that was co-founded by Duke University and the FDA, the Clinical Trials Transformation Initiative (CTTI). CTTI sought to develop and drive adoption of DCT practices by releasing their recommendations in 2018. These recommendations covered DCT approaches and protocol design in brief, as well as telemedicine state licensing issues, drug supply chain, mobile healthcare providers, investigator delegation and oversight, and safety monitoring.
The opportunities brought by DCTs were further explored by a multi-stakeholder consortium supported by EU/EFPIA Innovative Medicines Initiatives (IMI), namely Trials@ Home, which had as common goal the development of in-depth recommendations and pilot tools supporting widespread acceptance and use of remote DCTs in Europe. Trials@Home issued their first deliverables in 2020, and since then they have completed several reports that are spread throughout six work packages, each of which focused on investigating solutions and developing practical recommendations for the adoption of DCTs on the following six topics: (1) best practices in DCTs; (2) technologies—barriers, enablers, and data management; (3) a pan-EU remote DCT pilot; (4) ethical, regulatory, good clinical practices (GCP), and legal aspects; (5) communication, dissemination, and stakeholder engagement; and finally, (6) project management and synthesis.
The Association of Clinical Research Organizations (ACRO) is another organization dedicated to promoting clinical trial innovation and efficiency. It brings together CROs and technology companies to support optimization and development of new methodologies affecting DCTs. In 2020, ACRO developed a DCT toolkit in order to support and advance the adoption of decentralized trials, which includes five resources: (1) a detailed Quality by Design (QbD) manual for DCTs; (2) an accessible, quick-reference QbD manual; (3) a risk assessment considerations template; (4) DCT data flow maps; and (5) a change management question-and-answer (Q&A) resource. In addition to the DCT Toolkit, ACRO’s White Paper provides an overview of key issues in the decentralization of clinical trials and includes case studies from ACRO members.
One last organization worth mentioning is the Digital Medicine Society (DiMe), which tackles digital medicine involving the different fields of medicine, healthcare, and technology by generating best practices and guiding principles for accelerating clinical research and enhancing clinical care. They promote the use of digital medicine through the development of tools for measurement and intervention to support the practice of medicine broadly. Their library includes a large number of projects and resources categorized by four topics: digital measures; health care and public health; regulatory science; and publications. DiMe’s Playbook of Digital Clinical Measures addressed the processes for digital clinical measures and technologies used for remote monitoring in clinical trials, clinical care, and in public health settings.
Regulatory framework
The existing legal framework on clinical trials with medicinal products and associated guidelines do not prohibit the conduct of decentralized trials in general, but few of them provide advice on the use of specific decentralized elements (e.g., remote recruitment, digital endpoint selection) and trial-related interventions outside the trial site (e.g., digital consent, electronic data collection systems, electronic consultations).
The first regulations to provide recommendations for performing remote activities during the conduct of a clinical trial were issued during the COVID-19 pandemic. In March 2020, the World Health Organization (WHO) declared a COVID-19 pandemic for which no specific treatment existed at that time. COVID-19 had a large impact on the performance of traditional clinical trials due to quarantine measures, travel restrictions, and supply chain interruptions that led to patient trial participation discontinuation or withdrawal, unavailability of the clinical trial staff, site closures, and shortages of investigational medicinal products (IMPs). The degree of impact was different between the countries and regions, as this was depended on the implementation of the pandemic prevention measures at the national level as a response to the public health emergency. Thus, the decentralization of clinical trials started to gain attention and needed to be adopted within the regulatory framework. Given the impact of COVID-19 on traditional clinical trials, as well as the critical need for developing new COVID-19 treatments, regulatory agencies were forced to issue guidelines on clinical trial management during this time period.
Under these circumstances, the European Medicines Agency (EMA) released the Guidance on the Management of Clinical Trials during the COVID-19 (coronavirus) Pandemic to limit the disruption of clinical research during COVID-19 in the European region, which supported a harmonized approach among European (EU) Member States (MS) even though the local or national requirements prevailed in case of conflicting requirements. DCT-related elements introduced by this guideline were: conversion of trial participants’ physical visits into phone or video visits; contacting the trial participants via phone or video calls; obtaining written consent or approvals by email or mail; direct distribution of IMP to trial participants’ homes; transfer of trial participants to another trial site closer to their homes; trial participants testing in local laboratories; remote centralized and site monitoring activities; remote source data verification; and remote audits. The FDA also issued guidance for the conduct of clinical trials of medical products during the COVID-19 Public Health Emergency, with recommendations similar to the EMA guidance and additional details such as practice examples and Q&A that provide readers with more clarity.
The COVID-19-related guidelines and the specific exemptions granted during this pandemic are effective until the COVID-19 outbreak has passed. Moreover, EMA advised sponsors managing clinical trials impacted by the war in Ukraine to use the experience gained during the COVID-19 pandemic and apply the approaches and flexibilities agreed in this context.
Although the EU guideline on the management of clinical trials during COVID-19 is still effective, a few EU agencies issued national guidance on the DCT implementation to cover the continuous conduct of remote activities and to provide guidance on the safe implementation of DCT elements without compromising the safety and rights of trial participants or the integrity of the clinical trial. At the end of 2021, the Danish regulatory agency issued a guidance on the implementation of decentralized elements in clinical trials based on the knowledge gained from the close collaboration with clinical trial sponsors which conducted a small number of pilot projects with sub-elements of decentralized clinical trials that challenged the traditional framework. At the beginning of 2022, the Swedish regulatory agency published its recommendations on the decentralized trials based on the experience gained during a pilot project where five interventional clinical trials, representing all phases and both academic and commercial sponsors, were approved.
The recent and most-awaited joint EMA/ European Commission (EC)/Heads of Medicines Agencies (HMA) Recommendation Paper on Decentralized Elements in Clinical Trials was released in December 2022. The recommendation paper addressed the roles and responsibilities of the sponsor and investigator, electronic informed consent, IMP delivery, trialrelated procedures at home, data management, and monitoring in a decentralized clinical trial setting. Additionally, an overview of the current national requirements applicable in each relevant EU country has been provided in relation to the general recommendations of this paper.
The future of clinical trials decentralization
As noted above, COVID-19 has increased awareness of DCT, and the use of digital methods was a necessity for many trials to allow their continuation. This experience increased knowledge of using DCT elements, on which the industry and regulatory current recommendations presented above were based. This situation led to an increased interest in using DCT elements in clinical trials.
In May 2020, Informa Connect surveyed clinical trial professionals from different types of organizations on the adoption of DCT and related technologies, indicating that DCT adoption will increase faster in North America than elsewhere, as shown in Image 3.
Likelihood of increasing DCT within next two years
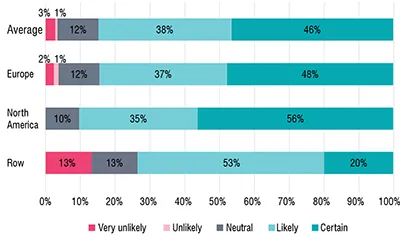
Image 3. Likelihood of increasing DCT
Although the DCT approach provides several benefits compared to conventional trials, there are still disadvantages and challenges to be considered when this new approach is considered. Currently, full remote trials are rarely conducted, and some of the DCT's elements may not be suitable for adoption in some trials. Nevertheless, the majority of trials can benefit from digitalizing trial components and switching to off-site or remote activities. However, the ability to adapt to the technological advances and to manage them should be considered, along with the recognition of the decentralized elements that are likely to have a significant impact on scientific validity, data integrity, the benefit-risk ratio, or the protection of trial participants’ rights. The key challenges facing DCT adoption are presented in Image 4 as per the Informa Connect 2020 survey.
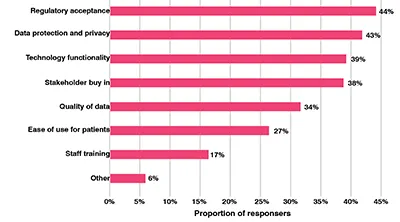
Image 4. DCTs biggest challenges
Among these challenges, the Informa Connect 2020 survey showed that the data protection and privacy challenge is hindering DCTs, especially in Europe as the GDPR framework is more restrictive than other data practices and that the quality of data is a more frequent challenge in the rest of the world as presented in Image 5.
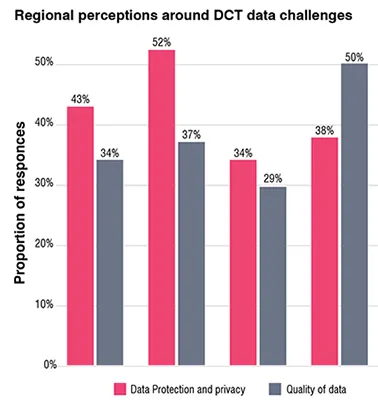
Image 5. Regional perceptions around DCT data challenges
Industry recommendations and best practices
Decentralization is the future of clinical trials, and as this is getting more attention, there is a need for clear and in-depth recommendations for implementing DCT elements, especially to address the challenges DCTs bring as presented above.
CTTI has developed a vision for how clinical trials should be done in 2030, following the following five views: (1) clinical trials are patient-centered and easily accessible; (2) clinical trials are fully integrated into health processes; (3) clinical trials are designed with a quality approach; (4) clinical trials maximally leverage available clinical and nonclinical data, including data collected via digital technologies, to minimize the collection of necessary trialspecific data; (5) clinical trials contribute knowledge about how to prevent, diagnose, and treat disease, and clinical trials are one of many sources of information that can be acted upon to improve population health. The ways of reaching this vision will need to be further investigated, and CTTI recognizes that some aspects will likely happen sooner than others, particularly in some countries.
Trials@Home is a five-year project, and the Trials@Home consortium continues to define and identify best practices for the DCT's conduct by completing the ongoing or not yet started deliverables contained in their six work packages. Based upon project activities that explore the methodological, technical, ethical, legal, regulatory, and practical aspects of implementing remote DCTs, they will publish their final recommendations in 2024.
Regulatory framework
Although COVID-19 has increased awareness of DCT, there is still a gap in understanding, experience, and familiarity with this concept. Different regulatory requirements at the national level also complicate the submission of multi-state trial applications. To support the industry, regulatory authorities would need to develop a long-term regulatory framework to address the complexity of DCTs and the continuous technological advances.
The International Council for Harmonization (ICH) GCP guideline update to revision 3 (R3) is a work in progress for which a draft version has been made available. The revision addresses the application of GCP principles to the new diverse trial types and data sources, and facilitates the use of technological innovations in clinical trials. To the ICH GCP (R3) will be added Annex 1 to address interventional clinical trials, and Annex 2 to provide any needed additional considerations for non-traditional interventional clinical trials. The adoption of the technical document is anticipated for December 2023.

Accelerating Clinical Trials in the EU (ACT EU), a joint EMA/EC/HMA clinical trials transformation initiative, was launched in January 2022 with the goal of better integrating clinical research in the European health system and strengthening the European environment for clinical trials, while maintaining a high level of data protection and robustness.
EMA has issued a draft Guideline on computerized systems and electronic data in clinical trials that will replace the current guideline Reflection paper on expectations for electronic source data and data transcribed to electronic data collection tools in clinical trials. A new guideline has been needed to address the complexity of computerized systems that have rapidly evolved in the clinical research environment during the last few years, from eCRFs and ePROs to various wearable devices (including instruments, software, and services) that are used in the creation and capture of electronic clinical data and in the control of other processes in the conduct of a clinical trial. The use of artificial intelligence (AI) will be further elaborated on in a future annex to this guideline.
The FDA Oncology Center of Excellence (OCE) supports efforts to modernise clinical trials through their collaboration with CTTI to conduct sponsor surveys to understand the prevalence of remote trial modifications for trials that provided evidence supporting the approval of supplemental or new drug or biologic applications for oncology indications.
FDA provided draft guidance for industry, investigators, and other stakeholders on digital health technologies for remote data acquisition in clinical investigations. This guidance outlines recommendations for use in clinical investigations that address the following topics: selection of digital health technologies (DHTs); verification and validation of DHTs; use of DHTs to collect data for trial endpoints; identification of risks associated with the use of DHTs; and management of risks related to the use of DHTs. The contents of this document intend to facilitate the use of DHTs in a clinical trial.
Conclusion
Clinical trial decentralization was not a widely implemented approach before the COVID-19 pandemic, despite the benefits this may bring. The transition from traditional clinical trials to DCTs has been forced in the context of the pandemic in order to support further clinical research on the IMPs. Decentralization has been adopted in a few trials where the partially remote approach has been preferred due to the challenges faced by the quick shift from on-site to remote trial activities. The current industry and regulatory framework provide guidance in support of decentralization, and it is expected that more companies involved in clinical trial research will implement decentralized elements and practices. To facilitate the employment of decentralization, the industry is encouraged to share their real-world experiences with DCTs and to closely collaborate with regulatory authorities to address both the successes and the challenges they faced. Decentralization of clinical trials is rapidly developing, and the continuous improvement of best practices promotes DCT adoption.
References:
[1] FDA. Digital Health Technologies for Remote Data Acquisition in Clinical Investigations. Draft Guidance for Industry, Investigators, and Other Stakeholders (Draft). Jan 2022. Link: Guidance for Industry (fda.gov). Last accessed: Dec 19, 2022.
[2] CTTI. CTTI Recommendations: Decentralized Clinical Trials. Sep 2018. Link: CTTI Recommendations: Decentralized Clinical Trials (ctti-clinicaltrials.org). Last accessed: Dec 19, 2022.
[3] Trials@Home. D1.1 First set of recommendations for RDCTs. Aug 26, 2020. Link: Trials@Home_D1.1-First-set-of-recommendations-for-RDCTs-to-be-implemented-in-the-pan-EU-pilot-RDCT.pdf (trialsathome.com). Last accessed: Dec 19, 2022.
[4] Craig H. Lipset. Decentralized Trials in the Digital Era: "Rethinking Hybrid". Jun 27, 2020. Link: Decentralized Trials in the Digital Era: “Rethinking Hybrid” (slideshare.net). Last accessed: Dec 19, 2022.
[5] Trials@Home. Deliverables. Link: Deliverables – Trials@Home (trialsathome.com). Last accessed: Dec 19, 2022.
[6] ACRO. Decentralized Clinical Trials Toolkit. Link: Decentralized Trials – ACRO (acrohealth.org). Last accessed: Dec 19, 2022.
[7] DiMe. Resources Library. Link: Access Resources – Digital Medicine Society (DiMe) (dimesociety.org). Last accessed: Dec 19, 2022.
[8] EMA. Guidance on the Management of Clinical Trials During the Covid-19 (Coronavirus) Pandemic. Version 5. Feb 10, 2022. Link: https://health.ec.europa.eu/system/files/2022-02/guidanceclinicaltrials_covid19_en_1.pdf. Last accessed: Dec 19, 2022.
[9] FDA. Conduct of Clinical Trials of Medical Products During the COVID-19 Public Health Emergency. Aug 30, 2021. Link: Conduct of Clinical Trials of Medical Products During COVID-19 Public Health Emergency (fda.gov). Last accessed: Dec 19, 2022.
[10] EMA. Advice to sponsors on managing the impact of the war in Ukraine on clinical trials. Mar 30, 2022. Link: Advice to sponsors on managing the impact of the war in Ukraine on clinical trials | European Medicines Agency (europa.eu). Last accessed: Dec 19, 2022.
[11[ Danish Medicine Agency. The Danish Medicines Agency’s guidance on the implementation of decentralized elements in clinical trials with medicinal products. Version 2.0. Sep 2021. Link: 5A96356760ED408CBFA9F85784543B53.ashx (laegemiddelstyrelsen.dk). Last accessed: Dec 19, 2022.
[12] Swidish Medical Products Agency. Decentralised and virtual interventional clinical trials. Last updated: Jan 17, 2022. Link: Decentralised and virtual interventional clinical trials | Swedish Medical Products Agency (lakemedelsverket.se). Last accessed: Dec 19, 2022.
[13] EMA/EC/HMA. Recommendation Paper on Decentralized Elements in Clinical Trials. Version 01. Dec, 2022. Link: mp_decentralised-elements_clinical-trials_rec_en.pdf (europa.eu). Last accessed: Dec 19, 2022.
[14] Informa Connect. Clinical Trials Europe - Decentralized Clinical Trials In 2020: A Global Survey. Global research study into adoption and technologies. July 21, 2020.
[15] CTTI. Transforming Trials 2030. Link: ctti_transforming_trials_2030_02042021.pdf (ctti-clinicaltrials.org). Last accessed: Dec 19, 2022.
[16] ICH. E6 Good Clinical Practice (GCP) Explanatory Note. Apr 19, 2021. Link: ICH_E6-R3_GCP-Principles_Draft_2021_0419.pdf. Last accessed: Dec 19, 2022.
[17] EMA/EC/HMA. ACT EU multi-annual workplan 2022-2026. Link: act-eu-multi-annual-workplan-2022-2026_en.pdf (europa.eu). Last accessed: Dec 19, 2022.
[18] EMA. Guideline on computerised systems and electronic data in clinical trials (Draft). EMA/226170/2021. Jun 10, 2021. Link: Draft guideline on computerised systems and electronic data in clinical trials (europa.eu). Last accessed: Dec 19, 2022.
[19] FDA. Advancing Oncology Decentralized Trials Modernizing Evidence Generation. Link: Advancing Oncology Decentralized Trials | FDA. Last accessed: Dec 19, 2022.