Curcumin’s Role as an Anti-Neurofibrillary Agent Towards Alzheimer's Disease
Sabrina Ruoyao Chen Zhang, Pharmacist, Massachusetts College of Pharmacy and Health Sciences University, Boston
Ronny Priefer, Dean of Graduate Studies, Massachusetts College of Pharmacy and Health Sciences University, Boston
Alzheimer’s disease is a progressive neurodegenerative disease that afflicts millions of people globally. Symptoms typically present as memory loss and cognitive decline. Existing hypthoses focus on the amyloid beta plaques and neurofibrillary tau tangles. In 2021, the only successful, albeit controversial, Alzheimer’s disease drug received FDA approval. Although this could/should demonstrate a fantastic medical achievement, the cost of this biologic may leave millions without access. Much research in the arena of natural products has shed light on the potential application of curcumin, specifically towards the neurodestructive tau tangles.
Curcumin is a natural, orange-yellow constituent of turmeric, the Indian spice derived from the plant Curcuma longa, belonging to the family of ginger. For centuries turmeric has been used in Asian culinary, textile, cosmetic, medicinal industries, as well asa preservative of food. Curcumin has been extensively evaluated for its biologic activity; exhibiting anti-inflammatory, oxidant, microbial, malarial, cancer,and Alzheimer effects. Hence, curcumin has been investigated to bea potential remedy to many malignant and non-malignant illnesses, such as diabetes, allergies, nephrotoxicity, AIDS, arthritis, cardiovascular disease, inflammation, and neurodegenerative diseases1. However, curcumin is characterized as a PAIN (pan-assay interference compound) and an IMP (invalid metabolic panaceas), which often complicatesin vitro and in vivoresults, leading to false positive outcomes2.
Some epidemiological studies have indicated that India has one of the lowest prevalence rates of Alzheimer’s disease in the world, coincidently while also having a high curcumin diet3. It has thus been postulated that this could be related to the food intake of this population, specifically, the aforementioned curcumin.
Alzheimer’s disease
Alzheimer’s disease is a progressive, age dependent neurodegenerative disease and the most common form of dementia. It is characterized by progressive neuronal loss and a decline in cognitive function that can ultimately affect behavior, mood, visuospatial orientation, and language, as well as impair memoryand some motor skills4. As of 2021, there were over 6 million Americans living with Alzheimer’s disease, with a projected rise to 13 million by 2050, due to the increase in life expectancy5.
Currently, the only therapeutic small molecular agents on the market targetting Alzheimer’s disease, work by temporarily reducing the cognitive symptoms of the disease. These are either cholinesterase inhibitorsorN-methyl-D-aspartate (NMDA) receptor antagonists. Many potential drugs have entered clinical trials in hopes to reverse the cognitive decline, howeverall have failed to show statistically significant reduction in the progression of the disease. The main hallmark signs of Alzheimer’s disease are: (1) the presence of beta amyloid plaques outside of neuron cells and (2) neurofibrillary (tau) tangles (NFTs) formation inside the cell6. Recently, the FDA approved aducanumab (Aduhelm®), a human monoclonal antibody directed against Aβ for the treatment of AD7.
The amyloid precursor protein (APP) is a transmembrane protein which is found in high levels in the brain. As it catabolizes, the non-amyloidogenic pathway is achievedvia α- then γ-secretase. However, in the amyloidogenic pathway, APP is cleaved by β- then γ-secretase, producing insoluble 39-42 amino acid peptide fragments, known as amyloid-beta (Aβ)8. Accumulations of Aβ peptides form beta amyloid plaques between neuronal cells, and disrupting signaling, eventually leading to cell death (Figure 1A).9 Amyloid-beta plaques may also lead tothe activation of immune cells that trigger inflammation.
Conversely, located in the neurons on the surface of the microtubules, tau proteins enhance the packing structure of the cytoskeleton. The over-activation of kinases lead toits hyperphosphorylation, decreasing biological activity,and ultimately theformation of neurofibrillary tangles.10 This lack of stable tau proteins weakens the microtubule integrity, leading to loss of signaling functionand ultimately cell death (Figure 1B).9
A) 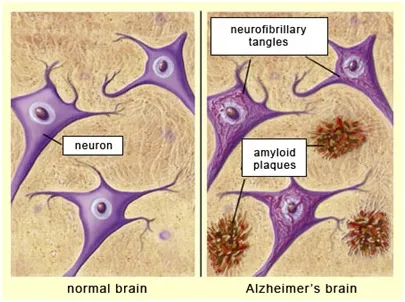
B) 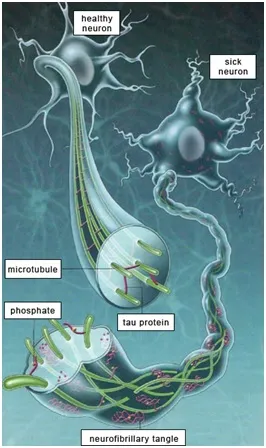
Fig. 1 (A & B): Amyloid beta plaques and neurofibrillary (tau) tangles. [9]
Various reports have shown that curcumin is a neuroprotective agentand can inhibit both the formation of amyloid oligomers and neurofibrillary tangles. Herein, is a review of various studies that have evaluated curcumin as a promising therapeutic agent for the treatment or prevention of Alzheimer’s disease focusing specifically on the tau cascade hypothesis.
Curcumin and tau
Tau aggregates are found in Alzheimer’s disease’s brains as an abnormal phosphorylated form, as pairedhelical filaments (PHFs), which can aggregate to form neurofibrillary tangles (NFTs)11. Rane et al.evaluated curcumin with regards to the aggregation of tau,and thus as a potential strategy for treating Alzheimer’s disease.12 Dynamic light scattering and atomic force microscopy revealed that curcumin did indeed inhibited NFTs. Furthermore, the disaggregation of tau suggested that curcumin assisted in dissolving preformed tau aggregates and filaments. Similary, Park et al. investigated the neuroprotective mechanisms by which curcumin acts against tau hyperphosphorylation in rat pheochromocytoma cells.13 Treatment of cells with curcumin prior to the introduction ofAβ, significantly decreased the amount of tau tangles by 40%. This suggested that curcumin worked by dissolving the phosphoryled tau that was induced by Aβ.
Recently, Patil et al.studieda library of polyphenols, one of which being curcumin, for the possible activity two endogenous proteins, BAG2 and LAMP1, which have been shown to play a vital role in clearing tau tangles from neurons.14 It was observed that treatment with curcumin efficiently countered induced tau hyperphosphorylation by 60% post treatment, witha 40% reduction for both pre-treatment and co-treatment in comparison to a control of, okadaic acid-induced pathological hyperphosphorylation of tau. Further, Bustanjiet al. demonstrated that curcumin is a potent inhibitor of glycogen synthase kinase-3β (GSK3β) which is involved with neuronal cell development.15
Additionally, Okuda and colleagues proposed that curcumin derived compounds could be more effective in treating Alzheimer’s diseasethan curcumin due to the latter having a poor blood-brain-barrier permeablilty profile.16 The group synthesized curcumin derivatives and screened them as dual inhibitors on Aβ and tau cascades. Assay results revealed that some of these analogues mainted in reasonable concentrations in the brain at 3 hours after oral administration and were potent inhibitorswith a superior pharmacokinetic profile.
Outlook
With the ever growing need for treatments/cures/prevention of Alzheimer’s disease, coupled with the aging global population, tapping into natural product knowledge and research may not only be scientifically reasonable, but necessary. Although the recent FDA approval of the first true Alzheimer’s disease drug in 2021 may help many, it is cost prohibitive for many more. Thus, looking to mother nature, may ultimately be the wisest path forward.
References
- Aggarwal, B. B., Sundaram, C., Malani, N., & Ichikawa, H. (2007). Curcumin: the Indian solid gold. The molecular targets and therapeutic uses of curcumin in health and disease, 1-75.
- Nelson KM, Dahlin JL, Bisson J, Graham J, Pauli GF, Walters MA. The Essential Medicinal Chemistry of Curcumin. J Med Chem. 2017;60(5):1620-1637.
- Mishra, S., &Palanivelu, K. (2008). The effect of curcumin (turmeric) on Alzheimer's disease: An overview. Annals of Indian Academy of Neurology, 11(1), 13.
- DeTure, M. A., & Dickson, D. W. (2019). The neuropathological diagnosis of Alzheimer’s disease. Molecular neurodegeneration, 14(1), 1-18.
- Liu, J., Hlávka, J., Hillestad, R. J., &Mattke, S. (2017). Assessing the preparedness of the US health care system infrastructure for an Alzheimer's treatment. RAND.
- Ashrafian, H., Zadeh, E. H., & Khan, R. H. (2020). Review on Alzheimer's disease: inhibition of amyloid beta and tau tangle formation. International journal of biological macromolecules.
- FDA. FDA Grants Accelerated Approval for Alzheimer’s Drug. FDA Website. June 7, 2021. Accessed August 22, 2021. https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-drug.
- Sadigh-Eteghad, S., Sabermarouf, B., Majdi, A., Talebi, M., Farhoudi, M., &Mahmoudi, J. (2015). Amyloid-beta: a crucial factor in Alzheimer's disease. Medical principles and practice, 24(1), 1-10.
- https://sphweb.bumc.bu.edu/otlt/mph-modules/ph/aging/Aging6.html (Accessed 10 June 2021)
- Brion, J. P. (1998). Neurofibrillary tangles and Alzheimer’s disease. European neurology, 40(3), 130-140.
- Brunden KR, Trojanowski JQ, Lee VM. Evidence that non-fibrillar tau causes pathology linked to neurodegeneration and behavioral impairments. J Alzheimers Dis. 2008;14(4):393-9.
- Rane JS, Bhaumik P, Panda D. Curcumin Inhibits Tau Aggregation and Disintegrates Preformed Tau Filaments in vitro. J Alzheimers Dis. 2;60(3):999-1014. doi: 10.3233/JAD-170351.
- Park SY, Kim HS, Cho EK, et al. Curcumin protected PC12 cells against beta-amyloid-induced toxicity through the inhibition of oxidative damage and tau hyperphosphorylation. Food ChemToxicol. 2008;46(8):2881-7. doi: 10.1016/j.fct.2008.05.030
- Patil SP, Tran N, Geekiyanage H, Liu L, Chan C. Curcumin-induced upregulation of the anti-tau cochaperone BAG2 in primary rat cortical neurons. NeurosciLett. 2013;554:121-5. doi: 10.1016/j.neulet.2013.09.008
- Bustanji Y, Taha MO, Almasri IM, Al-Ghussein MA, Mohammad MK, Alkhatib HS. Inhibition of glycogen synthase kinase by curcumin: Investigation by simulated molecular docking and subsequent in vitro/in vivo evaluation. J Enzyme Inhib Med Chem. 2009;24(3):771-8. doi: 10.1080/14756360802364377.
- Mohorko N, Repovs G, Popović M, Kovacs GG, Bresjanac M. Curcumin labeling of neuronal fibrillar tau inclusions in human brain samples. J NeuropatholExp Neurol. 2010;69(4):405-14. doi: 10.1097/NEN.0b013e3181d709eb.
Sabrina Zhang is a PY3 student pharmacist at the Massachusetts College of Pharmacy and Health Sciences – Boston. Her research interests include the effects of curcumin on patients with Alzheimer's disease.

Ronny Priefer, PhD is the Dean of Graduate Studies at the Massachusetts College of Pharmacy and Health Sciences University-Boston and a Full Professor of Medicinal Chemistry with almost 100 peer-reviewed publications. Additionally, he is a serial entrepreneur, with five start-up companies and over half a dozen patents.